In overhead athletes—especially baseball throwers—the subscapularis is often overlooked when diagnosing shoulder pain. Yet as the strongest rotator cuff muscle, it plays a critical role that, when compromised, can derail an entire season.
The Unsung Hero of Shoulder Stability
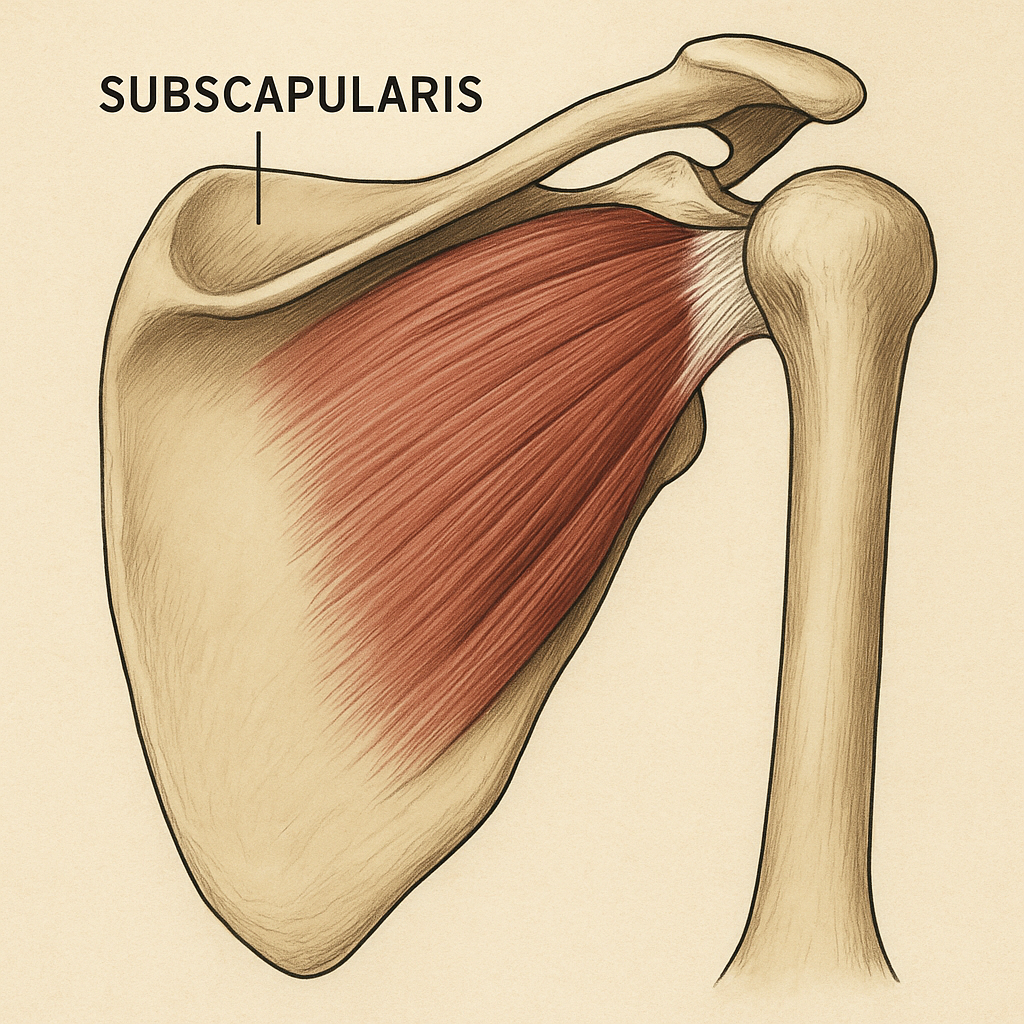
As the strongest rotator cuff muscle, the subscapularis plays a key role in internal rotation and, more importantly, in centering the humeral head in the glenoid during dynamic movement. When the subscap becomes dysfunctional, the humeral head may begin to glide forward or superiorly, increasing mechanical stress on the labrum, capsule, and surrounding tissues.
This isn't just about strength—it's about precision. The subscapularis acts as the primary dynamic stabilizer of the shoulder joint, working constantly to maintain optimal joint positioning during the explosive movements of throwing.
Why It Gets Overlooked
The subscapularis lies deep under the scapula and ribcage, making it difficult to palpate and assess. Its symptoms often mimic other conditions, leading to misdiagnosis and delayed treatment.
The Telltale Signs: More Than Just Shoulder Pain
One common but underappreciated symptom is radiating pain to the lateral deltoid, often felt in a straight line. This presentation can easily be mistaken for subdeltoid bursitis, an inflammatory condition of the bursa that cushions between the rotator cuff and acromion.
However, there are key differences in presentation that can help differentiate between the two:
Subscapularis Injury
- • Sharp, movement-triggered pain
- • Pain during internal rotation
- • Discomfort during follow-through
- • Pinpoint lateral deltoid pain
- • Instability sensations
- • Pain with reaching across body
Subdeltoid Bursitis
- • Diffuse, aching pain
- • Pain with overhead movement
- • Night pain when lying on side
- • Gradual onset of symptoms
- • Stiffness in morning
- • Pain with arm elevation
The Biomechanical Reality of Throwing
It's important to understand that during pitching, the shoulder experiences high distraction forces—literally pulling the ball out of the socket. The subscapularis plays a crucial role in resisting these forces, especially during deceleration.
During the late cocking and acceleration phases of throwing, the shoulder joint experiences forces that can exceed 1,000 Newtons of distraction. The subscapularis, working in concert with the other rotator cuff muscles, must fire precisely to maintain joint stability while allowing for the explosive internal rotation needed for velocity.
If the subscapularis is compromised, the shoulder's ability to stay stable under these massive loads drops significantly. This creates a cascade of compensations that can affect the entire kinetic chain.
⚠️ The Danger Zone
Playing through a subscap injury is dangerous. It can lead to chronic instability, labral tears, and eventual surgery. The longer it goes untreated, the more complex the rehabilitation becomes.

The explosive throwing motion places enormous demands on the subscapularis to maintain shoulder stability during deceleration
The Treatment Challenge
Because the subscap lies deep under the scapula and ribcage, it's difficult to rehab without precise manual therapy and motor control retraining. This isn't a muscle you can simply strengthen with traditional exercises—it requires a sophisticated approach.
The Treatment Hierarchy:
Rest and Activity Modification
Immediate cessation of aggravating activities to prevent further tissue damage
Trigger Point Release
Targeted manual therapy to address subscapularis trigger points and restore tissue quality
Restore Scapular Upward Rotation
Addressing scapular positioning to optimize subscapularis length-tension relationships
Serratus Anterior Strengthening
Essential for repositioning the scapula and re-establishing functional shoulder mechanics
Motor Control Retraining
Progressive loading and movement pattern correction to restore optimal function
Safe Trigger Point Techniques: Proceed with Caution
When addressing subscapularis trigger points, it's crucial to understand that you're working in a region dense with neurovascular structures. The axillary area contains the brachial plexus, axillary artery, and numerous lymph nodes—all of which require a respectful, gentle approach.
⚠️ Critical Safety Guidelines
- • Never use aggressive pressure in the axillary region
- • Avoid direct pressure on pulsing structures (axillary artery)
- • Stop immediately if numbness or tingling occurs
- • Work gradually—tissue changes take time
- • Consider referring to a qualified manual therapist
The subscapularis can be accessed through the axilla (armpit), but finding the right spot requires anatomical knowledge and a gentle touch. The muscle lies deep to the latissimus dorsi and teres major, making precise palpation challenging even for experienced practitioners.
Self-treatment with tools like lacrosse balls or massage devices should be approached with extreme caution in this area. What feels like muscle tension might actually be nerve irritation, and aggressive treatment can worsen symptoms or create new problems.
💡 Tool Recommendation (Ad)
If you're looking for a safer self-treatment option, the Acumobility Ball offers more controlled pressure and better ergonomics than traditional lacrosse balls. Its design allows for more precise targeting while reducing the risk of applying excessive force to sensitive areas.
*This is an affiliate link. I may earn a small commission if you purchase through this link, at no additional cost to you.
Prevention: The Best Medicine
The key to preventing subscapularis injuries lies in maintaining optimal scapular mechanics and addressing movement compensations before they become problematic. This includes:
- Regular assessment of scapular positioning and movement quality
- Maintaining adequate posterior shoulder flexibility
- Strengthening the serratus anterior and lower trapezius
- Addressing any thoracic spine mobility restrictions
- Monitoring training loads and recovery
The Bottom Line
If a thrower reports pinpoint deltoid pain or instability, the subscapularis deserves your attention—before it's too late. Early recognition and appropriate treatment can mean the difference between a few weeks of modified activity and months of rehabilitation.
When to Seek Help
Don't wait for the pain to become unbearable. If you're experiencing any combination of lateral deltoid pain, instability sensations, or pain during internal rotation movements, it's time to get a proper assessment.
The subscapularis may be hidden from view, but its impact on shoulder function is anything but subtle. Recognizing its importance and addressing dysfunction early can keep you throwing strong for years to come.